Abstract
A 28-year-old male presented with chronic low back pain persisting for two years following a civilian gunshot injury, with retained shrapnel fragments in the L2 vertebra. Despite multiple outpatient evaluations and extensive pharmacological treatments, including nonsteroidal anti-inflammatory drugs, gabapentinoids, antidepressants, and opioids, his pain remained inadequately controlled. Due to the presence of retained spinal foreign bodies, epidural interventions were avoided. As an alternative approach, an ultrasound-guided erector spinae plane block (ESPB) was performed at the T12 level. The patient experienced immediate and significant pain relief, with sustained improvement in pain scores, mobility, and quality of life. During a one-year follow-up period, no complications or recurrence of symptoms were observed, and the patient did not require additional analgesic interventions. This case highlights ESPB as a safe and effective option for managing chronic post-traumatic low back pain in patients with retained spinal fragments, particularly when conventional interventional techniques are contraindicated.
Keywords: spinal gunshot wound, chronic post-traumatic pain, regional anesthesia, erector spinae plane block, pain management
Introduction
Chronic pain management in patients with retained bullet fragments in the spine remains a significant clinical challenge. Gunshot wounds to the spine can lead to persistent pain even in the absence of neurological deficits, making treatment decisions complex. While surgical removal of bullet fragments is considered in cases of neurological compromise, instability, or infection, its role in pain management alone remains controversial.1,2
The erector spinae plane block (ESPB) is a novel regional anesthetic technique that has been widely utilized for the management of thoracic and lumbar pain. Unlike epidural injections, ESPB offers a safer alternative by delivering analgesia at a site remote from the primary pathology, reducing the risk of complications such as infection or neurological injury. Recent studies have demonstrated its efficacy in acute postoperative pain, trauma cases, and chronic back pain. However, to our knowledge, this is the first report describing ESPB for chronic post-traumatic pain due to retained spinal shrapnel, highlighting its potential in cases where other interventional options are contraindicated.3
This case report presents a patient with chronic low back pain due to retained shrapnel in the spine, successfully treated with ESPB. The report highlights the effectiveness of ESPB as a pain management strategy and discusses its advantages over traditional approaches in patients with foreign bodies in the spine.
Case Presentation
Two years after sustaining a civilian gunshot wound to the lower back, a 28-year-old male presented to the emergency department with a civilian gunshot wound to the lower back. Neurosurgical evaluation revealed shrapnel fragments in the right transverse process of the L2 vertebra and adjacent paravertebral muscles. Given the absence of neurological deficits, conservative management was initiated. However, he experienced persistent low back pain, which progressively worsened over the first three months and then stabilized at 5–6/10 on the Visual Analog Scale (VAS).
He attended multiple outpatient visits and was prescribed various analgesics, including NSAIDs, tramadol, gabapentin, pregabalin, and selective serotonin reuptake inhibitors (SSRIs; specifically sertraline), with minimal relief. Additionally, he developed gastric side effects. Two years post-injury, he presented to our outpatient clinic with similar complaints and declined further use of adjuvant medications for chronic pain. Non-pharmacological interventions had also been attempted, but with no significant improvement.
Neurological examination revealed normal motor strength (5/5) and intact deep tendon reflexes in both lower extremities. Sensory examination showed no hypoesthesia, allodynia, or dermatomal sensory loss. The straight leg raise test and femoral stretch test were negative bilaterally. Gait and coordination were unremarkable. However, the patient exhibited a compensatory right-sided trunk lean during ambulation, likely to offload pain from the left paravertebral region.
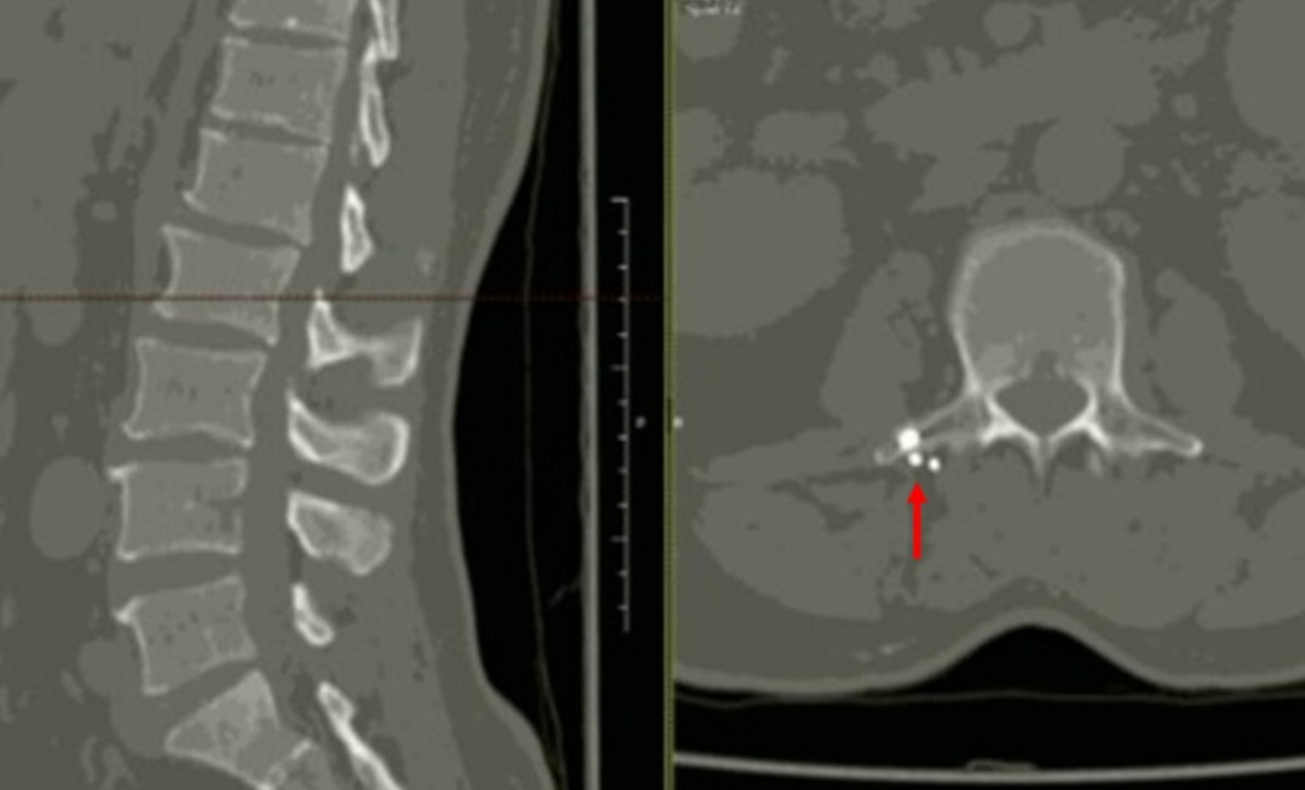
A well-healed scar was noted in the right lumbar region, 3 cm from the midline. Palpation of the paravertebral muscles overlying L2–L3 on the right side elicited sharp, localized pain rated 10/10 on the Visual Analog Scale (VAS). There were no signs of radiculopathy, myelopathy, or systemic infection. Blood work and imaging showed no biochemical evidence of lead toxicity. Lumbar computed tomography (CT) revealed multiple shrapnel fragments around the right transverse process of the L2 vertebra (Figure 1) without fractures or misalignment.
Due to the presence of retained foreign bodies in the spine and the associated infection risk, the patient had never received an epidural injection. He was referred to an anesthesiologist for evaluation of eligibility for an erector spinae plane block. After the discussion, the patient consented to a regional nerve block.
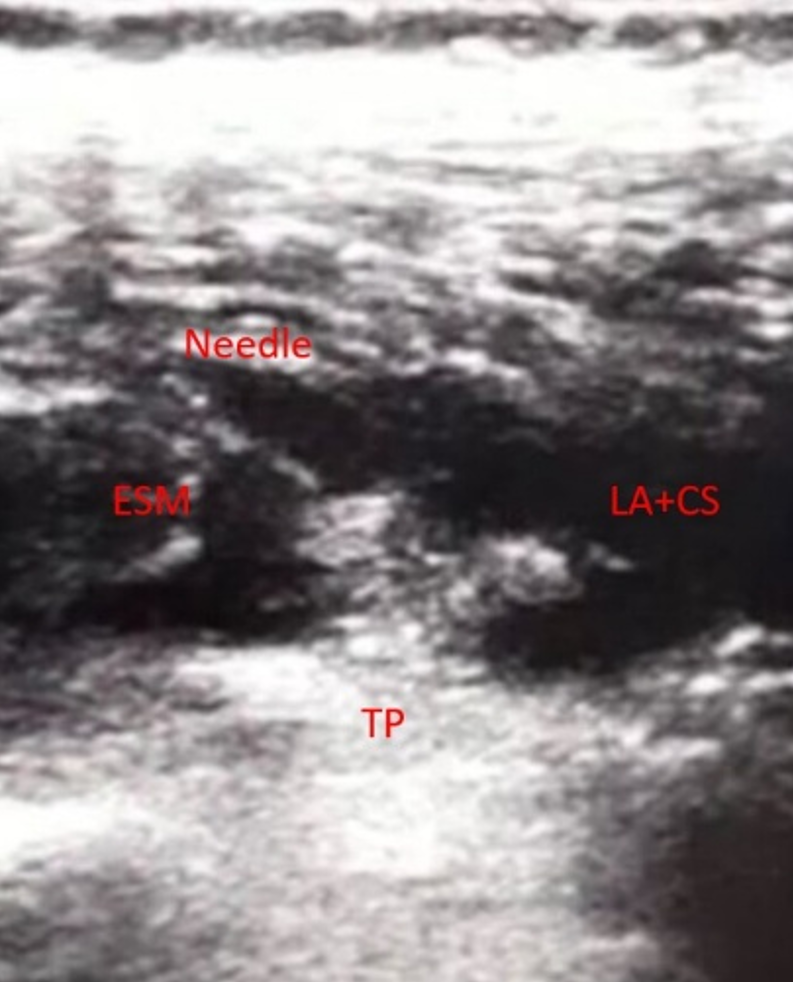
The patient received intravenous cefazolin (1.5 g) preoperatively and was positioned prone. A C-arm scope confirmed the T12 vertebral level. Following surgical skin preparation with chlorhexidine, a high-frequency ultrasound was placed in a longitudinal position, 3 cm to the right of the midline. After identifying the erector spinae muscle and the right transverse process of T12, a 10-cm, 18-gauge block needle was inserted into the interfascial plane between the transverse process and the erector spinae muscle. A total of 10 mL of 0.5% bupivacaine HCl mixed with 5 mL of long-acting corticosteroids was injected unilaterally along with 10 mL of sterile saline (0.9%) (Figure 2).
The procedure was uneventful, and the patient was discharged with paracetamol and oral amoxicillin-clavulanic acid three hours after the procedure. His hourly VAS scores were 3/10, 2/10, and 3/10, respectively. The patient was monitored post-procedure in the outpatient clinic. On postoperative day 3, his pain score on the Visual Analog Scale (VAS) was 1/10, compared to 10/10 at baseline. He reported a marked improvement in mobility and sleep quality. Follow-up evaluations were conducted monthly for a period of 12 months. At each visit, he maintained a VAS score of 0–2/10 and reported no recurrence of symptoms, no need for additional medications or procedures, and a return to his baseline level of physical activity. No adverse effects related to the ESPB or delayed complications (e.g., infection, motor deficits) were observed. He did not require any emergency visits or further specialist consultations during this period.
Discussion
The erector spinae plane block (ESPB) is a regional block technique initially described for chronic thoracic pain, including neuropathic and somatic components.3 Its indications have expanded to include not only chronic pain management but also acute postoperative pain following spine, orthopedic, and thoracic surgeries. Several reports have documented the use of ESPB in trauma patients. Ahiskalioglu et al. previously described a case where ESPB was successfully applied for bilateral lumbar transverse process fractures.4 Additionally, this technique has demonstrated efficacy in patients with traumatic rib fractures.5,6 Here, we report a case of intractable chronic pain caused by retained bullet fragments in the spine. To our knowledge, there are no previously reported cases similar to ours.
Although a definitive causal relationship between the retained shrapnel and the patient’s chronic pain cannot be proven without invasive diagnostics, the temporal onset, consistent localization, and reproducible pain with palpation over the L2 paravertebral region support a mechanical and possibly inflammatory origin linked to the foreign bodies. Imaging revealed retained metallic fragments in the right transverse process area, precisely beneath the site of maximal tenderness. Additionally, the absence of dermatomal symptoms, normal neurological findings, and the lack of spinal instability or other structural abnormalities on CT suggest that the pain was unlikely to originate from radiculopathy or segmental pathology. The marked and sustained response to a single-level ESPB targeting this region further supports a localized pain generator associated with the retained shrapnel. The clinical presentation was consistent with predominantly mechanical nociceptive pain, possibly with a myofascial component, rather than neuropathic pain.
The application of ESPB in spinal surgery as part of a multimodal analgesia regimen is a relatively new approach. Singh et al. reported significantly lower rates of blood loss and higher patient satisfaction in their study (blood loss: 5.1±3.17 vs. 57.70±5.90; p<0.001; patient satisfaction score: 9.52±0.65 vs. 8.22±0.79; p<0.001). Randomized controlled trials have also demonstrated reduced postoperative opioid consumption with ESPB use.7-9
Recently, Anshus et al. reported the use of ESPB in the emergency department (ED) for patients with chronic low back pain experiencing acute exacerbations. They observed significantly reduced VAS scores (81.5%) and a decreased length of stay in the ED (73.5 minutes), with most patients not requiring further ED admissions (5/6, 83%). Moreover, all study participants remained opioid-free during follow-up, suggesting ESPB as a promising technique for chronic low back pain management.10 Similarly, our patient did not require further hospital admissions for intractable pain, apart from scheduled outpatient follow-ups, and reported no significant pain thereafter.
Since local anesthetics spread to wider areas in ESPB, it can be performed without direct involvement of the primary pathology, unlike epidural injections. Previous studies have shown that local anesthetic diffusion extends across five vertebral levels.11 In a cadaveric study where ESPB was performed with methylene blue dye, no anterior spread was observed, indicating that no local anesthetic reached the ventral rami.12 Additionally, ESPB targets a site remote from neuraxial structures, offering a safer alternative to epidural injections.13 These clinical findings supported our decision to use ESPB in this case, as avoiding the primary pathology was particularly crucial given the retained foreign material in the spine.
The efficacy of ESPB in managing chronic pain can be attributed to both its anatomical spread and the pharmacodynamics of the agents used. Anatomically, the local anesthetic is deposited in the fascial plane deep to the erector spinae muscle, allowing cephalocaudal spread over multiple dermatomes and affecting both dorsal rami and, to a lesser extent, ventral rami through indirect diffusion. This broad coverage explains the block’s utility in cases involving diffuse or deep somatic pain. Pharmacologically, long-acting local anesthetics, such as bupivacaine, provide extended analgesia by inhibiting sodium channels in nociceptive fibers. The addition of corticosteroids contributes to anti-inflammatory effects and may potentially reduce ectopic neural discharge. This dual mechanism makes ESPB a compelling option in cases of complex spinal pain, including myofascial and possible neuropathic components, where conventional pharmacologic therapy alone proves insufficient. In previous reports, ESPB has provided relief lasting from weeks to several months for chronic pain, making the sustained one-year benefit in our patient particularly notable.14
Compared to other regional techniques such as paravertebral block (PVB) or epidural anesthesia, ESPB offers several practical and safety advantages. While PVB provides effective analgesia, it carries a higher risk of pneumothorax and technical complexity due to its proximity to the pleura and neuraxial structures. Epidural blocks, though effective, are often contraindicated in patients with retained foreign bodies or infection risk near the injection site. In contrast, ESPB is easier to perform under ultrasound guidance, has a lower complication rate, and achieves a wide craniocaudal spread of analgesia without penetrating deep into neurovascular structures. These features make it especially suitable for complex trauma cases or in patients where conventional blocks pose higher risks.15,16 Other potential interventions, such as paravertebral block, intercostal nerve block, or facet joint injections, were considered less suitable in this case due to the proximity of retained metallic fragments to the injection site, increasing the potential risk of infection or inadvertent contact with foreign bodies, as well as the broader dermatomal coverage required for adequate analgesia, which is more effectively achieved with ESPB.
The management of spinal gunshot injuries remains controversial.17 Neurological deterioration, instability, infection, and cerebrospinal fluid leakage are absolute indications for surgery. However, chronic pain without these factors presents a unique challenge for neurosurgeons.18 Furthermore, removing the bullet may not always provide pain relief.19Despite reports suggesting that bullet extraction or spinal cord stimulator implantation can alleviate chronic pain in select patients.20
In this case, the patient was not considered an ideal surgical candidate due to the small, numerous, and scattered nature of the bullet fragments. Before pursuing complex surgical interventions, a conservative approach is often preferred. Therefore, ESPB was chosen as a safe and effective alternative to manage his chronic pain.
This case report has several limitations inherent to its single-patient design, limiting generalizability and precluding comparison with other pain management strategies. Follow-up beyond one year was not available, restricting assessment of long-term durability. Placebo effects, regression to the mean, and natural symptom fluctuation cannot be excluded, although spontaneous improvement after prolonged chronic pain is uncommon. Nevertheless, the close temporal relationship between ESPB and pain relief, consistent pre-procedural pain localization, and sustained symptom resolution despite discontinuation of analgesic medications suggest a clinically meaningful treatment effect. Larger case series and controlled studies are required to further evaluate the efficacy and long-term outcomes of ESPB in chronic post-traumatic spinal pain.
Conclusion
Given the rarity of this application, ESPB may be considered a viable first-line regional analgesia technique in cases of chronic pain associated with retained spinal foreign bodies, particularly when epidural access is contraindicated. Future use may benefit from a standardized approach, including careful imaging to assess fragment location, use of ultrasound-guided needle placement at least two vertebral levels away from the pathology, and structured follow-up to evaluate long-term outcomes. Establishing a clinical registry or multicenter case series could help guide practice and inform safety protocols.
Written informed consent was obtained from the patient for the publication of this case report, including relevant medical details and accompanying images. All personal identifiers have been removed to ensure patient confidentiality in accordance with ethical standards.
Etik kurul onayı
Bu çalışma bir olgu sunumudur, bu nedenle etik kurul onayı gerektirmemektedir.
Yazarlık katkısı
Çalışma konsepti ve tasarımı: DDB, GO, AA; veri toplama: DDB, GO, AA; sonuçların analizi ve yorumlanması: DDB, CIG, DS, GO, AA; makaleyi hazırlama: CIG, DS, AA. Yazar(lar) sonuçları gözden geçirmiş ve makalenin son halini onaylamıştır.
Finansman
Yazar(lar), çalışmanın herhangi bir finansal destek almadığını beyan etmiştir.
Çıkar çatışması
Yazar(lar) herhangi bir çıkar çatışması olmadığını beyan etmiştir.
Ethical approval
This study is a case report, therefore does not require an ethics committee approval.
Source of funding
The authors declare the study received no funding.
Conflict of interest
The authors declare that there is no conflict of interest.
References
- Wang J, Lu Y. Application of ultrasound-guided bilateral erector spinae plane block in lumbar spinal surgery. Ann Palliat Med 2020; 9: 1282-1284. https://doi.org/10.21037/apm-20-287
- Ueshima H, Inagaki M, Toyone T, Otake H. Efficacy of the erector spinae plane block for lumbar spinal surgery: a retrospective study. Asian Spine J 2019; 13: 254-257. https://doi.org/10.31616/asj.2018.0114
- Tulgar S, Selvi O, Senturk O, Serifsoy TE, Thomas DT. Ultrasound-guided erector spinae plane block: indications, complications, and effects on acute and chronic pain based on a single-center experience. Cureus 2019; 11: e3815. https://doi.org/10.7759/cureus.3815
- Ahiskalioglu A, Kocak AO, Doymus O, Sengun E, Celik M, Alici HA. Erector spinae plane block for bilateral lumbar transverse process fracture in emergency department: a new indication. Am J Emerg Med 2018; 36: 1927.e3-1927.e4. https://doi.org/10.1016/j.ajem.2018.06.072
- Luftig J, Mantuani D, Herring AA, Dixon B, Clattenburg E, Nagdev A. Successful emergency pain control for posterior rib fractures with ultrasound-guided erector spinae plane block. Am J Emerg Med 2018; 36: 1391-1396. https://doi.org/10.1016/j.ajem.2017.12.060
- Gluncic V, Bonasera L, Gonzalez S, Lukić IK, Candido K. Combination of the T7 unilateral erector spinae plane block and t10 bilateral retrolaminar blocks in a patient with multiple rib fractures on the right and t10-12 vertebral compression fractures: a case report. Local Reg Anesth 2021; 14: 99-102. https://doi.org/10.2147/LRA.S312881
- Singh S, Choudhary NK, Lalin D, Verma VK. Bilateral ultrasound-guided erector spinae plane block for postoperative analgesia in lumbar spine surgery: a randomized control trial. J Neurosurg Anesthesiol 2020; 32: 330-334. https://doi.org/10.1097/ANA.0000000000000603
- Liu MJ, Zhou XY, Yao YB, Shen X, Wang R, Shen QH. Postoperative analgesic efficacy of erector spinae plane block in patients undergoing lumbar spinal surgery: a systematic review and meta-analysis. Pain Ther 2021; 10: 333-347. https://doi.org/10.1007/s40122-021-00256-x
- Yu Y, Wang M, Ying H, Ding J, Wang H, Wang Y. The analgesic efficacy of erector spinae plane blocks in patients undergoing posterior lumbar spinal surgery for lumbar fracture. World Neurosurg 2021; 147: e1-e7. https://doi.org/10.1016/j.wneu.2020.10.175
- Anshus AJ, Oswald J. Erector spinae plane block: a new option for managing acute axial low back pain in the emergency department. Pain Manag 2021; 11: 631-637. https://doi.org/10.2217/pmt-2021-0004
- Adhikary SD, Bernard S, Lopez H, Chin KJ. Erector spinae plane block versus retrolaminar block: a magnetic resonance imaging and anatomical study. Reg Anesth Pain Med 2018; 43: 756-762. https://doi.org/10.1097/AAP.0000000000000798
- Fusco P, DI Carlo S, Scimia P, Luciani A, Petrucci E, Marinangeli F. Could the new ultrasound-guided erector spinae plane block be a valid alternative to paravertebral block in chronic chest pain syndromes? Minerva Anestesiol 2017; 83: 1112-1113. https://doi.org/10.23736/S0375-9393.17.12109-7
- Ivanusic J, Konishi Y, Barrington MJ. A Cadaveric study investigating the mechanism of action of erector spinae blockade. Reg Anesth Pain Med 2018; 43: 567-571. https://doi.org/10.1097/AAP.0000000000000789
- Chin KJ, El-Boghdadly K. Mechanisms of action of the erector spinae plane (ESP) block: a narrative review. Can J Anaesth 2021; 68: 387-408. https://doi.org/10.1007/s12630-020-01875-2
- Ma G, Gou J, Chen L, Qiao X. Analgesic comparison of erector spinae plane block with intercostal nerve block for thoracoscopic surgery: a meta-analysis of randomized controlled trials. Medicine (Baltimore) 2023; 102: e35093. https://doi.org/10.1097/MD.0000000000035093
- Pang J, You J, Chen Y, Song C. Comparison of erector spinae plane block with paravertebral block for thoracoscopic surgery: a meta-analysis of randomized controlled trials. J Cardiothorac Surg 2023; 18: 300. https://doi.org/10.1186/s13019-023-02343-w
- Klimo P, Ragel BT, Rosner M, Gluf W, McCafferty R. Can surgery improve neurological function in penetrating spinal injury? A review of the military and civilian literature and treatment recommendations for military neurosurgeons. Neurosurg Focus 2010; 28: E4. https://doi.org/10.3171/2010.2.FOCUS1036
- Hakan T, Çerçi A, Gürcan S, Akçay S. Firearm bullet settling into the lumbar spinal canal without causing neurological deficit: a report of two cases. Surg Neurol Int 2016; 7: S251-S254. https://doi.org/10.4103/2152-7806.181978
- Waters RL, Sie IH. Spinal cord injuries from gunshot wounds to the spine. Clin Orthop Relat Res 2003; 408: 120-125. https://doi.org/10.1097/00003086-200303000-00014
- Keel JC, Lau ME, Gulur P. Spinal cord stimulation for radicular pain following retained bullet in the spinal canal. Pain Physician 2013; 16: E103-E106.
Copyright and license
Copyright © 2026 The Author(s). This is an open access article distributed under the Creative Commons Attribution License (CC BY), which permits unrestricted use, distribution, and reproduction in any medium or format, provided the original work is properly cited.